Answers of Multi-Layer Flow Modulator Multi-Layer Flow Modulator
Illness and prevalence about disease
An abdominal aortic aneurysm (AAA) is a bulge or swelling in the aorta, the main blood vessel that runs from the heart down through the chest and tummy. An AAA can be dangerous if it is not spotted early on. It can get bigger over time and could burst (rupture), causing life-threatening bleeding. Epidemiology — The prevalence of abdominal aortic aneurysm (AAA) is 4 to 8 percent in screening studies, affecting predominantly males [7-10]. However, AAAs found on screening are generally small; those measuring ≥5.5 cm or greater are found in only 0.4 to 0.6 percent of those screened.
Causes and symptoms of disease
Causes
Aneurysms can develop anywhere along the aorta, but most aortic aneurysms occur in the part of the aorta that's in the belly area (abdomen). Several things can play a role in the development of an abdominal aortic aneurysm, including:
- Hardening of the arteries (atherosclerosis). Atherosclerosis occurs when fat and other substances build up on the lining of a blood vessel.
- High blood pressure. High blood pressure can damage and weaken the aorta's walls.
- Blood vessel diseases. These are diseases that cause blood vessels to become inflamed.
- Infection in the aorta. Rarely, a bacterial or fungal infection might cause abdominal aortic aneurysms.
- Trauma. For example, being injured in a car accident can cause abdominal aortic aneurysms.
Symptoms
Abdominal aortic aneurysms often grow slowly without noticeable symptoms, making them difficult to detect. Some aneurysms never rupture. Many start small and stay small. Others grow larger over time, sometimes quickly.
If you have an enlarging abdominal aortic aneurysm, you might notice:
- Deep, constant pain in the belly area or side of the belly (abdomen)
- Back pain
- A pulse near the bellybutton
What is features of Multi-Layer Flow Modulator
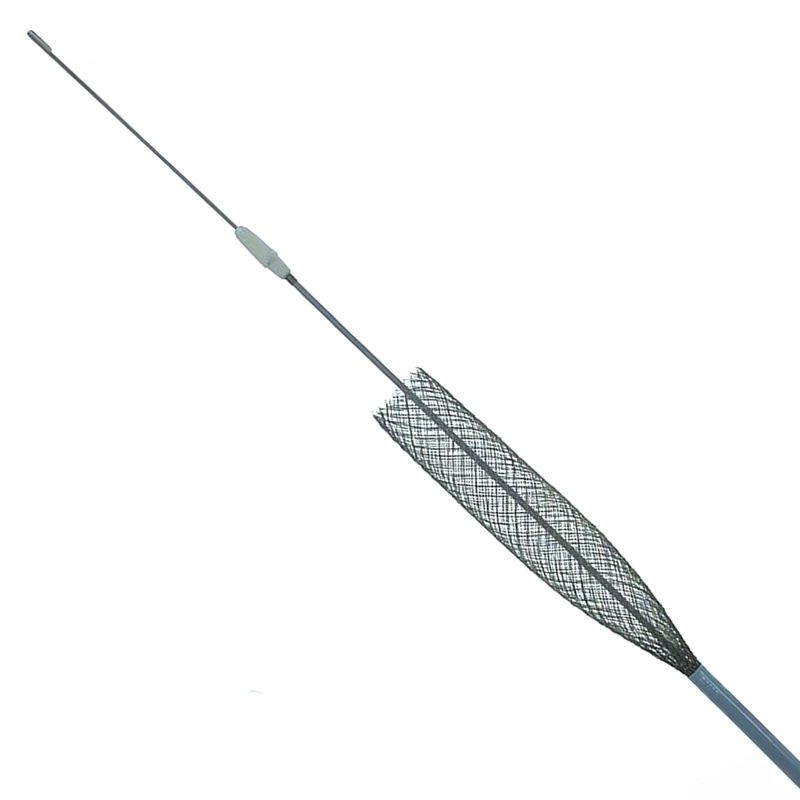
The stent is made of super alloyed biomedical wire with a self-expandable system, knitted in a multi-layer tubular mesh structure. This design structure allows the stent to be flexible, conformable, and self-expanding.
The delivery system is compatible with 18F and 20F size - 0.035" guidewire. Sheath Y is connected to the pusher through the hemostasis valve. When tightened, the sheath locks into the holder. This lock is required to prevent premature deployment of the multilayer current routing system.
The multilayer Stena® boots into the stent delivery system. Both are inserted percutaneously or by cutting down from the access artery (preferably the femoral artery) and advanced endoluminal to the desired lesion site under angiographic imaging.
- Provides restoration of healthy laminar blood flow
- Protects branch artery patency
- Organized stable thrombus formation
- Rapid endothelialization along the vessel wall
- The effective minimally invasive implantation procedure
- Radiopaque markers are made of tantalum at both ends.
- Compatible with 0.035” guide wire.
How to treat and cure process
Stena Stent use requires the administration of intravenous contrast material. Patients with pre-existing renal failure may be at increased risk of renal failure in the postoperative period. Care should be taken to limit the amount of contrast to minimize the risk of distal embolism and blood clotting: use systemic heparinisation.
Insert the 0.035” 300cm guidewire into the arteriotomy and advance it along the catheter up to the upper part of the aorta (proximal to the lesion). Remove the sheath with the flushing catheter while maintaining the guidewire position. If an introducer sheath is used, the size must be at least 20F.
Replace the delivery system on the guidewire.
Result and scientific studies
Between 2015 and 2020, a total of 61 patients with AAA, thoracoabdominal aortic aneurysm, or thoracic aortic aneurysm were treated with the MFM endograft in 29 hospitals. However, data from 40 patients with a mean age of 73.4 ± 11.2 years (72.5% male; 29/40) and a mean aortic aneurysm diameter of 60.3 ± 16.6 mm from 14 hospitals were available for this retrospective study. With a survival rate at 1 month, 6 months, and 12 months of 97%, 78%, and 70%, respectively. Freedom from failure mode (type I or II) at 1 month, 6 months, and 12 months was 97.5%, 88%, and 86%, respectively, and visceral vessel patency was 99.3% (155/156 available). Freedom from rupture and freedom from reintervention at 1 month, 6 months, and 12 months were 97.5% and 100%, 96% and 84%, and 86% and 75%, respectively.